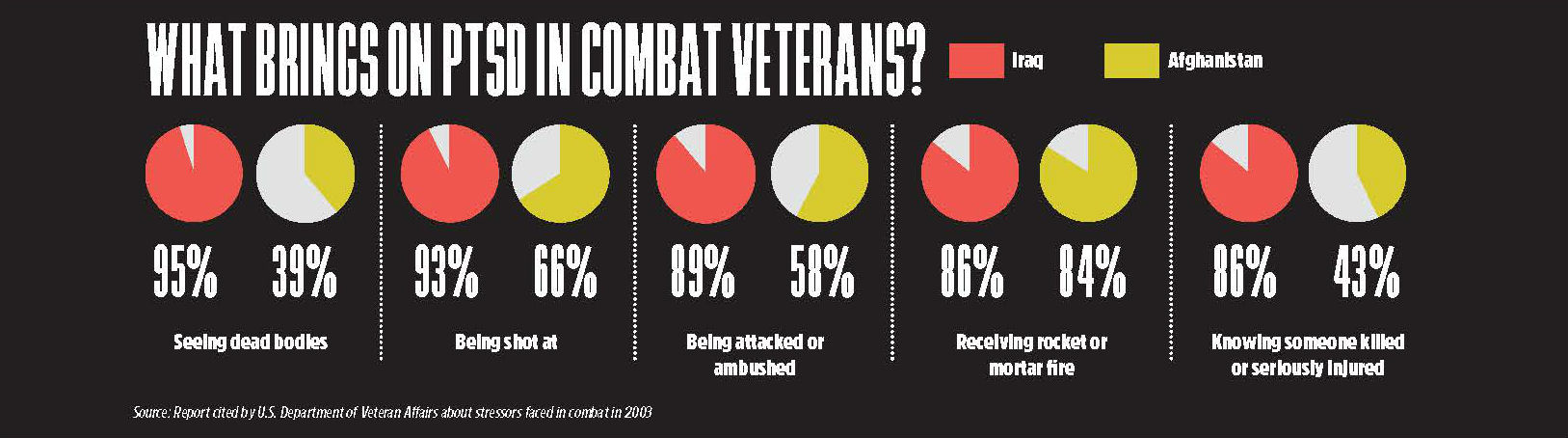
Iraq, 2003: Operation Iraqi Freedom begins. Brandon Wyatt, an 18-year-old paratrooper with the 82nd Airborne, was working with 11 million gallons of jet fuel at a forward air refueling site 20 miles outside the perimeter of his base camp. His job was to protect the fuel and distribute it to strategically important locations in 500-gallon inflatable drums.
The enemy had him and his team in their sights. They wanted to blow up this huge 11-million-gallon bomb Wyatt was guarding and kill every American soldier they could. So every night, the mortars would rain down on him. After three days, he would return to base, try to get some rest, then do it all again. Day after day, the same thing for 18 months. On alert. On edge. “Every night, I didn’t go to sleep,” he says. “Not one night.”
No human is built to sustain that over a long time in one setting, he told himself. “So what happens at the end of the experience is that you become nonfunctional because all of your systems are depleted. All of your tolerances are gone. And once your emotions are gone, once your fear is gone, once your longing for home is gone, once even your sense of right and wrong is gone, all you have left is survival.”
When his tour of duty was over, when his year and a half spent almost entirely in theater was done, he found that he was not able to process … anything. “I shut down,” he says. “I went mute. I didn’t talk.”
So he was shipped first to a hospital in Germany, then to another one in Savannah, Georgia, then eventually to Walter Reed Hospital for treatment of his diagnosed affliction: post-traumatic stress disorder. He was getting intensive psychological interventions and other treatments that were supposed to help. But his inability to talk made it worse. “They tried to help me with a lot of pills,” he says. “But I couldn’t talk. I couldn’t tell them that those pills weren’t working. So in my head, I would explode. The pills made me want to hurt myself, where before, I was scared of other people hurting me in Iraq because of the trauma of what I saw.”
So, he says, he started thinking about killing himself. “[I was] just sitting for hours focusing on just how to kill myself because of those things that my team and I saw for over a year and a half,” he says.
He was in a dark place. He didn’t trust the Army. He didn’t trust anyone. “What they did by leaving me out there in theater so long was just not right,” he says. “That was not what we were signed up for. That’s just torture.”
Wyatt’s story is the story of many returning combat veterans. They come home after months or years of deployment, ready to leave their experiences in war behind them, but face the dilemma of adjusting to the calm, orderly civilian life they left. They are now battle-tested warriors who have been deeply, irreversibly changed.
Military clinicians work with them, trying to do the right thing with what they think they know about PTSD. But they don’t always get it. Pills help but can end up causing more problems as vets get addicted, depressed, hopeless. Suicidal.
Popular therapies for PTSD are about reliving experiences instead of dealing with the present and with the future. New approaches are desperately needed because vets commit suicide at the rate of 22 a day.
“Up until recently, PTSD was classified as an anxiety disorder,” Crystal Shelton, vice president of clinical programs for Cohen Veterans Network, says. “It’s incredibly complex. When combat vets come back from deployment, they have a lot of issues because they have been away from their families for so long, or they missed the birth of a child. There are a lot of issues about reintegrating not only in the civilian world but in their family that can cause depression and any number of issues that are not necessarily PTSD.”
CVN, a chain of free mental-health clinics for war veterans, was founded in 2015 by billionaire hedge-fund manager Steven Cohen. He heard from his son, Robert, a Marine and 2010 Afghanistan vet, about the PTSD issues many returning vets had, which became Cohen’s inspiration for creating the network of clinics. The hope was to try to find new and better ways to treat PTSD. There are now five clinics across the country, with up to 20 more to come including in the Metro-D.C. area.
Shelton, who was part of a team that helped lead the first-ever mental health clinic at Wounded Warrior Battalion-East, says clinicians like her have developed interventions like prolonged exposure therapy and cognitive processing therapy that can help the combat vet make meaning through therapy. “But they can’t forget the grief for a dead buddy they experienced as a combat veteran or move away from it. It is a part of them,” she says. Therapy can reduce the hypervigilance most returning vets find hardest to deal with and help them find joy and pleasure in life again, she says. “Yes, there is meaning on the other side of combat, but we need to be open to the fact that there are no right answers.”
Dr. Amy Williams, a clinical psychologist who has been working in trauma and PTSD for over 20 years, is currently the clinic director of one of the CVN network clinics in Addison, Texas. “Not everybody that is exposed to a traumatic event is going to develop PTSD,” she says. “It comes about as a result of a life-threatening event, something that is shocking, that is big. It can happen to you or you can witness it. People go into fight-or-flight response, which is normal. Then when it’s over, they have to make meaning out of it.”
Some people who have social support can get over it and move forward, she says. But others simply get stuck. “They are just on guard, really vigilant, with a lot of emotions: anger, guilt, irritability and then avoidance.”
They don’t want to talk about it, which prolongs the problem. “But to treat it, you have to approach the trauma. You have to go there,” Williams says.
Most clinicians agree that treatment for PTSD is a moving target with no guaranteed results. In fact, according to a recent study published by the Journal of the American Medical Association, current clinical therapies do result in “meaningful improvements,” but many patients continue to have symptoms, and “there is a need for development and testing of novel evidence-based treatments.”

One of the more novel approaches to treating PTSD for combat vets being used now is in Bluemont, which has a population of about 3,000. Here, in a 37-acre rustic resort 50 miles west of Washington, D.C., in the foothills of the Blue Ridge Mountains, there is a rural, personal decompression and family reconnection paradise for returning combat veterans from any generation and conflict. It’s called Boulder Crest Retreat.
The retreat, which opened in September 2013 and has had 700 visitors each year, features four well-appointed three-bedroom cabins with a full-sized kitchen and a 52-inch TV with DirectTV in each. Outdoors, there is archery, horseback riding, cozy meeting areas and more. Everything is free.

BCR was founded by retired veteran Ken Falke and his wife, Julia. Falke, a former special forces soldier who specialized in finding and destroying bombs, was seriously wounded in 1989. He and his wife started a foundation to connect families with returning combat veterans in March 2013—the nonprofit Explosive Ordnance Disposal Warriors Foundation—which led to the creation of BCR on their farmland.
The retreat is about two core programs: family rest and reconnection. It’s designed to transition deep struggle into strength and make life more purposeful, according to Josh Goldberg, the director of strategy for BCR. “It’s about retraining the returning combat [veteran] to enter the civilian life he left, helping them process who they are now after experiences that no one but other combat veterans have seen or could understand,” he says.
BCR is led by executive director Dusty Baxley, an 82nd Airborne combat veteran, serving from 1972-1994 on multiple tours of duty. Baxley is also a transcendental meditation instructor at the retreat.
When Baxley’s tour of duty was over, he went directly to Australia and stayed there for 15 years. “But I missed my tribe,” he says. “I had no one to talk to and went off the rails. I reached the point where I had no value, so in 2009, I basically came home to die.”
He checked in with Veterans Affairs in Florida, where he moved, and says they didn’t even look up from their paperwork. They asked him some questions and gave him prescriptions for some opioids. “I thought, ‘This is great,’” he says. “‘These will go with my Wild Turkey perfectly.’”
So, he says, he proceeded to try to drink himself to death. But he began meditating and got better, eventually attracting the attention of Falke, who told him about his vision for BCR. Baxley came to BCR in April 2015. “I feel alive because I now have a mission and a purpose, and that is why I am here,” he says.
He is not a fan of the diagnosis of PTSD because he believes it is the medical community’s way of putting a label on something that makes it easier for them to work it through the bureaucratic system. “Those main PTSD symptoms are things that we are trained to have,” he says. “We are trained to be hypervigilant. We are trained to turn off our emotions. We are trained to not tolerate mistakes because if you make a mistake, I die. Our bodies are always on adrenaline all of the time. Then you come home, and that is still how you are, and that is not socially acceptable.”
He says that when the VA doctors told him he had PTSD, he felt like there was nothing wrong with him. “This combat experience is what happened to me, so I need to know what is going on here, in my brain, and here, in my heart, because the two things are disconnected. My heart is shut down.”
Baxley taught transcendental meditation before coming to BCR as a mentor, teacher and guide in the combat stress recovery retreats held there. “I finished teaching a meditation course in a medical center before coming to BCR, and a guy hung back. [He] shakes my hand, and there’s a bullet in my hand. I said, ‘What’s going on?’ He said, ‘I have been carrying this the entire course. If this didn’t work, I was going to eat this bullet,’” he says. “In five years here, I got a bag of those. They would say ‘This bullet’s yours, dude. I am back. You kept me from dying.’”
Another vet at BCR is James Ritchie, an Army paratrooper from 2003 to 2011. His first days back from his tour were equally disturbing. “I would be in a public place and walk through the front door and not feel safe,” he says. “I would actually walk an entire lap of the perimeter, learn all of the exits and the vantage points, and sit with my face facing the door. Then I was safe. As long as I had control of the environment I was in, I was safe. But in places like dance clubs where it was chaotic, I would be on edge and ready to fight.”
His outfit, the 173rd Airborne that invaded Iraq in 2003, experienced some of the highest casualties from the beginning of the war at that time. They lost 96 men in four deployments over a 40-month period. He found out that there were guys he knew committing suicide—18 suicides in 19 months—and felt like he had no choice but to join them. “It was, ‘Well, if my brothers can’t survive this situation, I am not going to survive it either.’ So I started living the gun-in-the-mouth blues.”
He says that when he came back from combat he was a “professional relationship killer.” “I was so comfortable in my own misery that when there was no misery, I would create it, and then it was a downward spiral,” he says.
When his wife left at the end of December 2015, he was at his lowest point. “I came to BCR as a beaten man, no longer in control of my destiny or my environment, and living in a bottle,” he says.
His first two days taking the combat stress retraining at BCR were rough. “A special forces buddy of mine said, ‘Imagine having your hands tied and your feet tied and [being] thrown into the deepest end of the swimming pool. You sink or swim. It’s your decision.’ And that is how the first two days were.” He got through the training, a job opened up at BCR in May 2016, and he took it.
His breaking point was working with the horses. “The horse will follow you if you are confident,” he says. “I wasn’t confident. Even though I jumped out of airplanes, survived 40 months of combat, did CrossFit marathons, I had no confidence.”
PTSD, he says, should just be PTS. “It’s combat stress. I would throw out the word disorder.”
Goldberg agrees that treating PTSD needs new and innovative approaches like those offered at BCR. “It’s counterintuitive that if you want to move forward you keep talking about the past,” he says. “What we do is train people to be able to live in the present and move forward.”
Can PTSD be cured? Wyatt says he found his cure: cannabis. “It was the first time it slowed my brain down a little and allowed me to sleep enough to have linear thought,” he says. He is now an attorney and an active supporter of the local chapter of Weed for Warriors, a growing organization of veterans that began in San Francisco and is spreading across the country. Their mission is to force the VA to allow cannabis for treatment of vets, something that has not happened yet, with more and more pressure from both advocates and the medical community as more states legalize medical marijuana. Congress denied funding for access to veterans again in September.
“‘Cure’ is always an interesting word to me,” Williams says. “Because when you ask someone who has been traumatized, maybe a cure to them is making it never have happened. And we can’t make it never have happened. You can process it and get better. But this still happened to you. You learn how to be stronger and can live a good life. So that to me is recovery.”
“You say recover. I say transcend,” Goldberg says. “There has to be an approach that leverages the innate trust that combat vets feel for each other. That is what we believe.”
People don’t need to be scared of vets with PTSD, Baxley says, because all that is really going on is a person who has been highly trained to endure and survive circumstances where his life was on the line each day for months or years and who needs to finally come to terms with a new, safe, forgiving and giving lifestyle. “Society needs to wipe off its glasses and realize that there is nothing wrong with us,” he says “This is who we are. We are your national fighting force. We go in harm’s way just for you and gain some skills and talents. There is knowledge to be gained from us.”
“You can never unsee what you saw,” Wyatt says. “You can change how you respond to it and change your ability to understand it. And you can also change the ability to use that to continue to be a hero in civilian life.”

Current treatments for PTSD
– Cognitive processing therapy. CPT involves 12 sessions of psychotherapy that teach a patient how to evaluate and change upsetting thoughts a patient has had since their trauma.
– Prolonged exposure therapy. The goal is to have less fear about memories. It is based on the idea that people learn to fear thoughts, feelings and situations that remind them of a past traumatic event. By talking about the trauma repeatedly with a therapist, a patient will learn to get control of their thoughts and feelings about the trauma and not be afraid of their memories. A patient may also be guided to practice different ways to relax when having a stressful memory, such as using breathing exercises.
– Eye movement desensitization and reprocessing therapy. While thinking of or talking about stressful memories, the patient is asked to focus on other stimuli like eye movements, hand taps and sounds.
– Prescription drugs. Selective serotonin reuptake inhibitors are a type of antidepressant medicine designed to help a patient feel less sad and worried. SSRIs include citalopram (Celexa), fluoxetine (such as Prozac), paroxetine (Paxil) and sertraline (Zoloft).